Emergency Room Guide · Fabric Health
Making an app for the hardest room in the hospital.
I joined Fabric Health as the sole designer on ERG — Emergency Room Guide — to help ER patients, nurses, and providers navigate a visit together. Across six months it reached 5,700 patients at three hospitals and saved nurses 5–10 minutes per intake. But the thing I'm proudest of isn't on the dashboard.
Company
Fabric Health (formerly Florence)
Product
ERG · Emergency Room Guide
Role
Lead & sole Product Designer
Team
Product Designer, Product Manager, Tech Lead, Integrations Dev, Chief Clinical Officer
Timeline
2022 — 2023
Shipped to
3 hospitals including a pediatric ER
The Brief
Fabric Health wanted to buy a hospital and rebuild it from first principles.
The problem
Problem 1
Patients had no signal in the chaos.
Before ERG, an ER visit meant: check in, sit down, wait two or three hours with no idea where you are in the process, whether you've been forgotten, or what's coming next.
Problem 2
Nurses had no time to capture context.
Intake was verbal, repetitive, and happened in the worst possible conditions. Nurses re-asked the same questions, chased paper, and documented by exception.
Problem 3
Discharge had no next step.
Patients left without a Primary Care Provider attached, which meant many came back to the same ER for the same reason a month later. A cost driver for the hospital, and a worse outcome for the patient.
Research
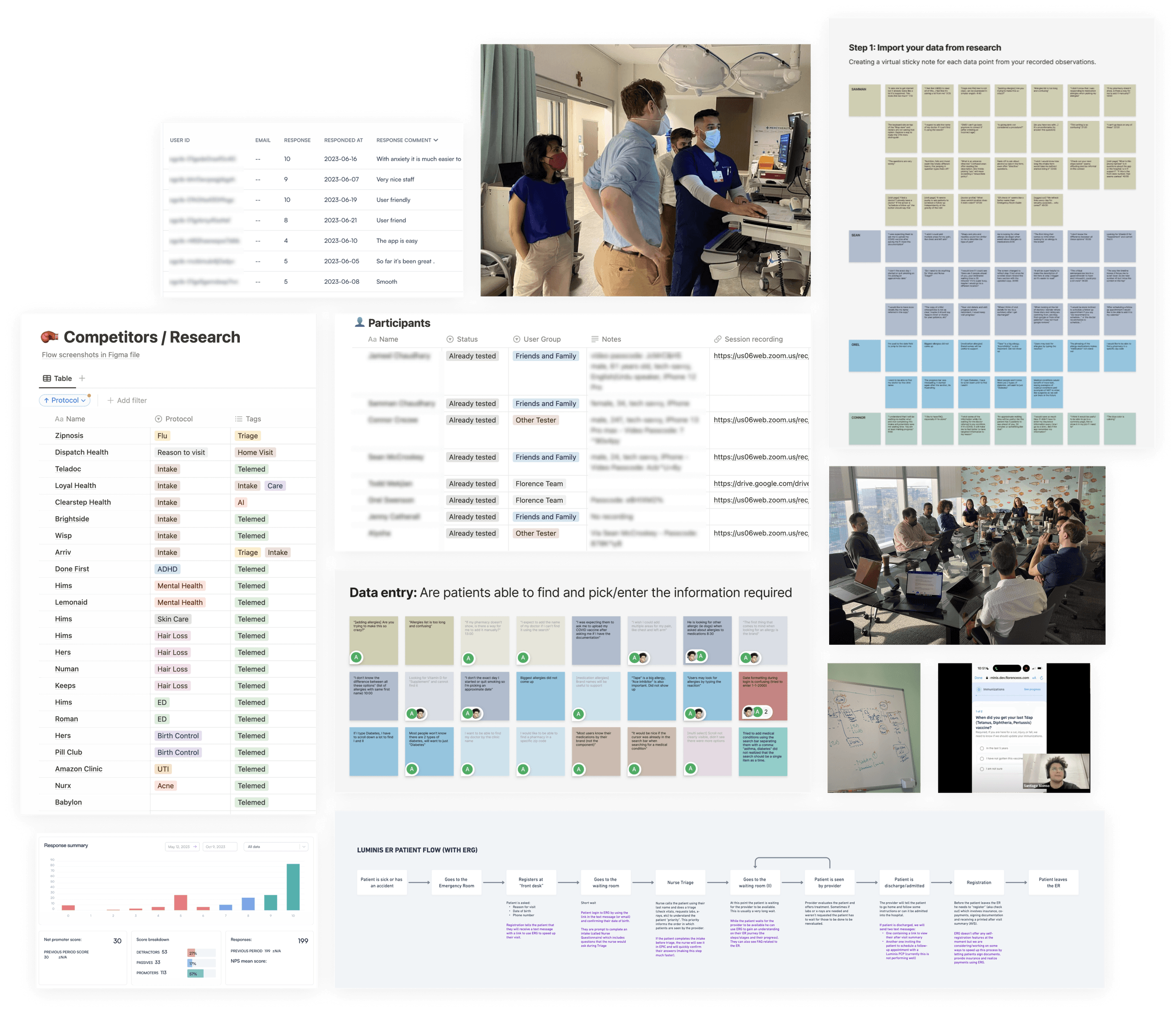
I went to the ER. Not as a designer but as a visitor.
As the sole designer on a product built for the ER, I couldn't work from a Figma file alone. I spent time at the hospital, walked the full patient journey, and did a shift in the pediatric ER to understand how the same product had to behave when the user is a parent comforting a sick toddler.
Observation 01
Patients aren't anxious because of the wait. They're anxious because they don't know if the wait is working.
Observation 02
Nurses aren't following a script. They're running decision trees in real time. One answer can skip ten questions and add two more.
Observation 03
Pediatric triage is a different environment, with parents as proxies and a completely different emotional floor.
Observation 04
The ER is chaotic by need, those who are more critical get seen first. That makes it almost impossible to predict anything.
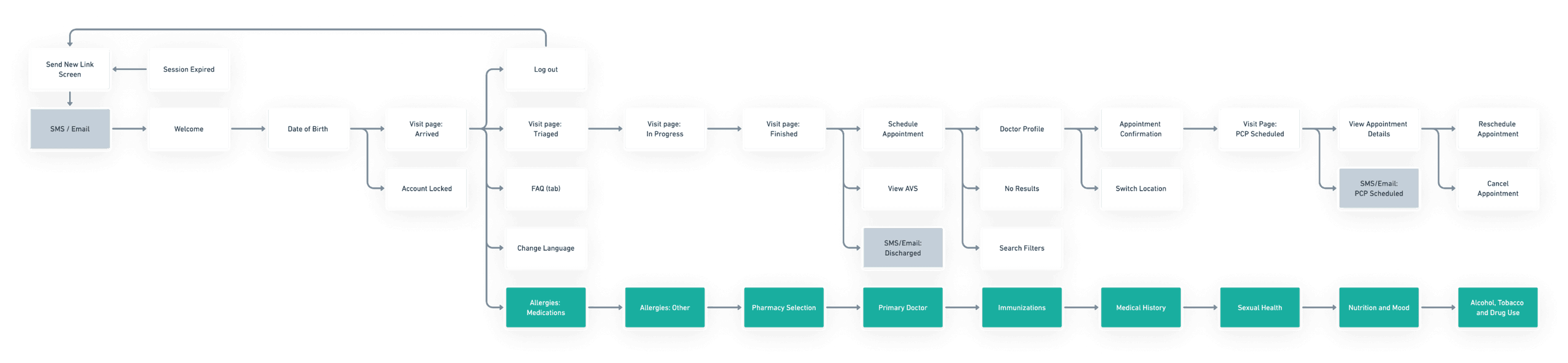
Mapping the experience
From verbal intake to a dynamic decision engine.
The first version of ERG was focused on one thing: replacing a verbal, paper-based intake with a dynamic questionnaire that could branch, skip, and adapt based on patient answers. Before designing any UI, I mapped the decision tree the nurses were running in their heads.
Benefit 01
Patients stop waiting and start doing. A dynamic intake on their phone makes the wait feel like progress is being made.
Benefit 02
Nurses get their time back. Low-acuity intake moves to the patient, freeing nurses to focus on the people who need them most.
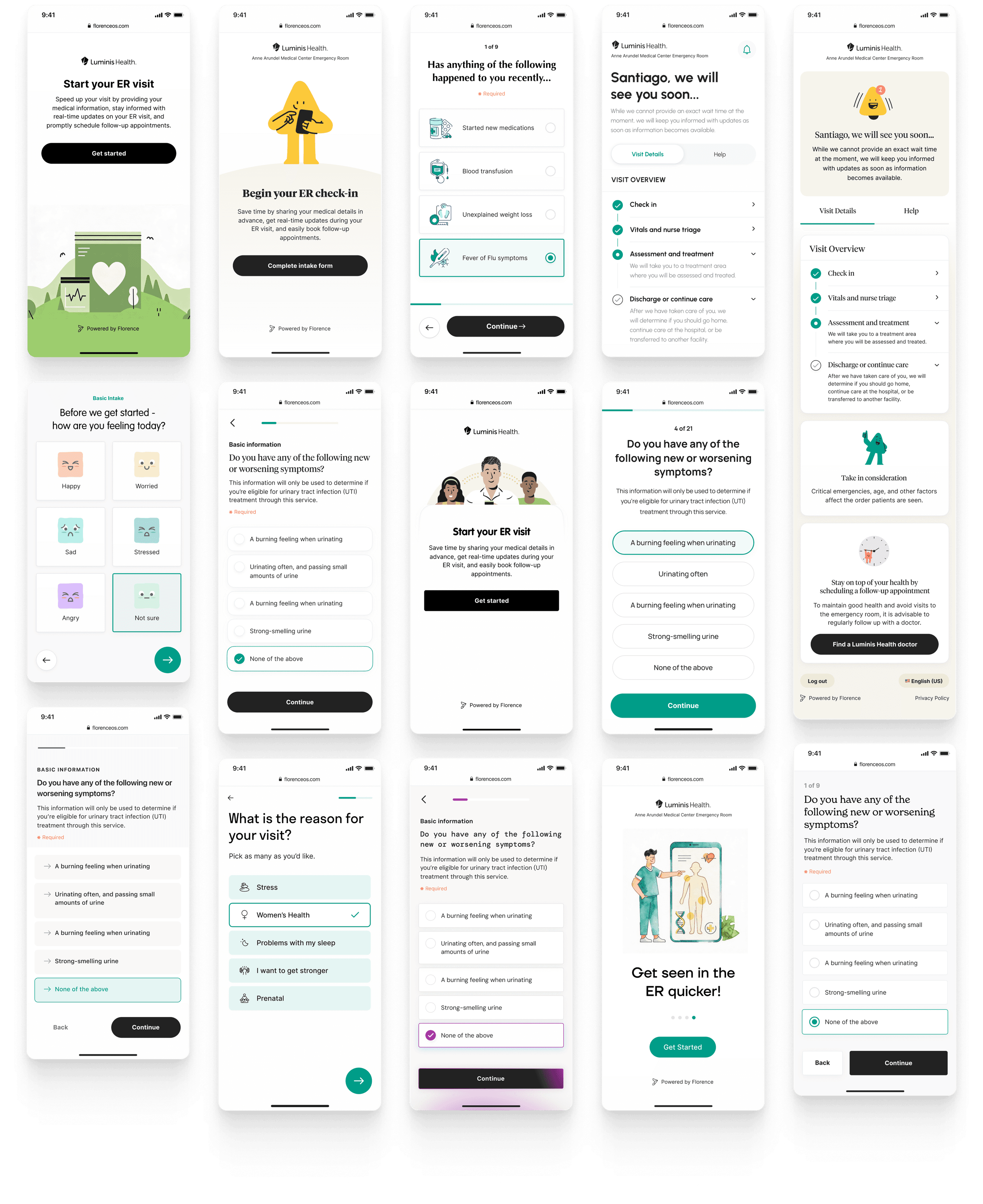
Design exploration
Visual exploration toward a calmer voice.
The hospital aesthetic is loud by default — red badges, warning icons, dense forms. ERG had to feel like the opposite: calm, clear, considered. The exploration narrowed on a soft green-white palette that signaled health without shouting.
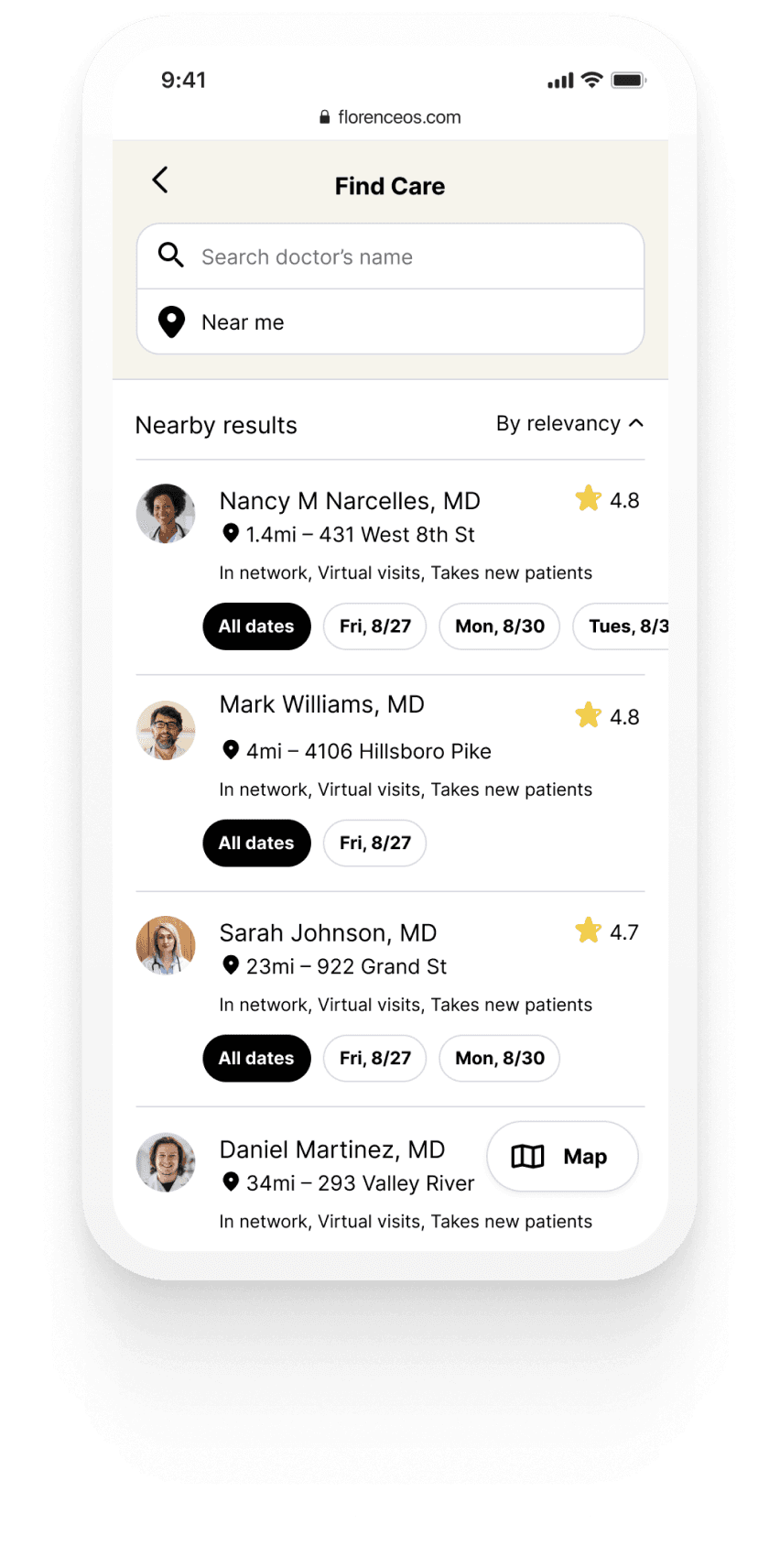
01 · Answers → Patients in crisis can't parse long flows
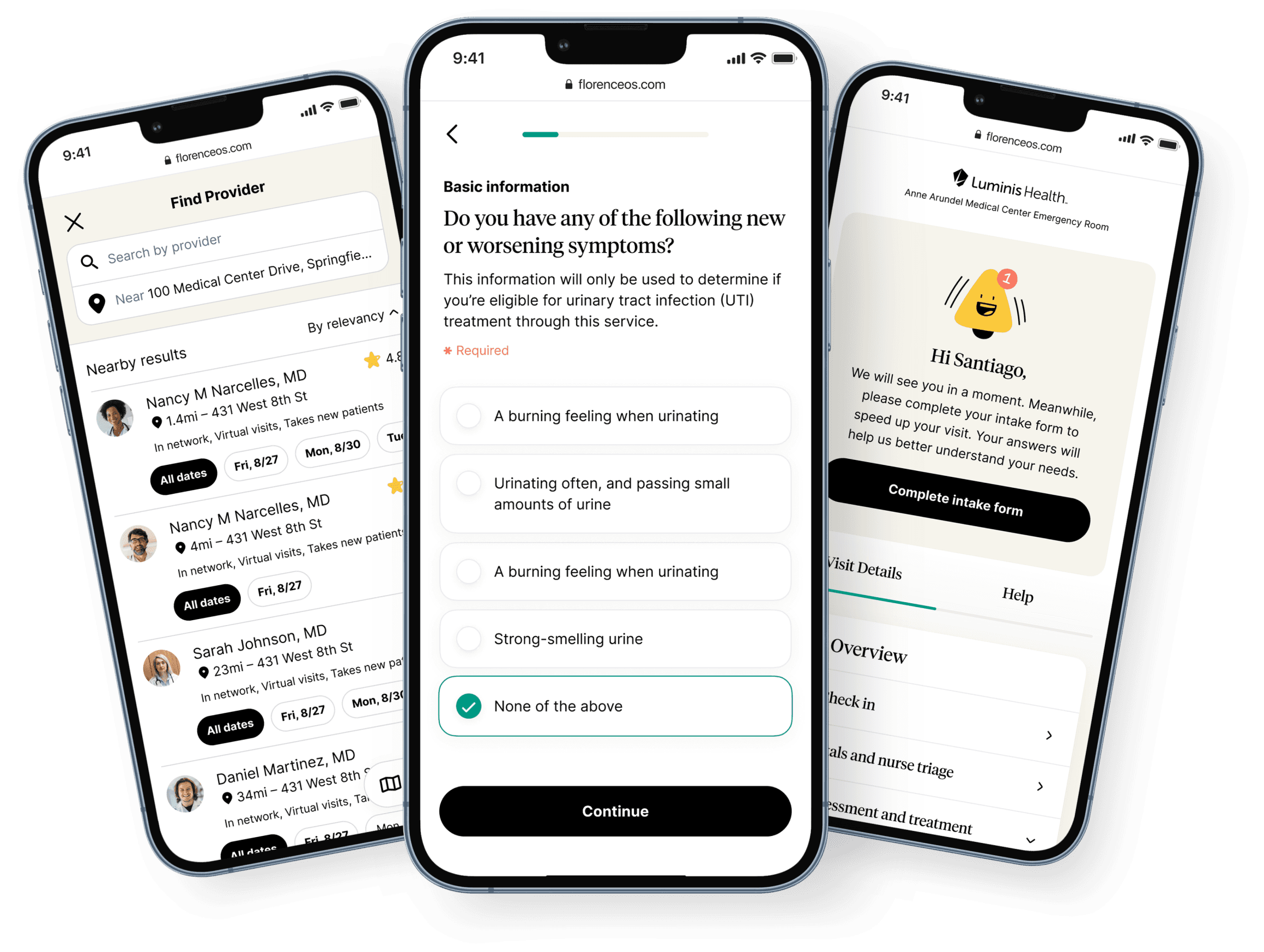
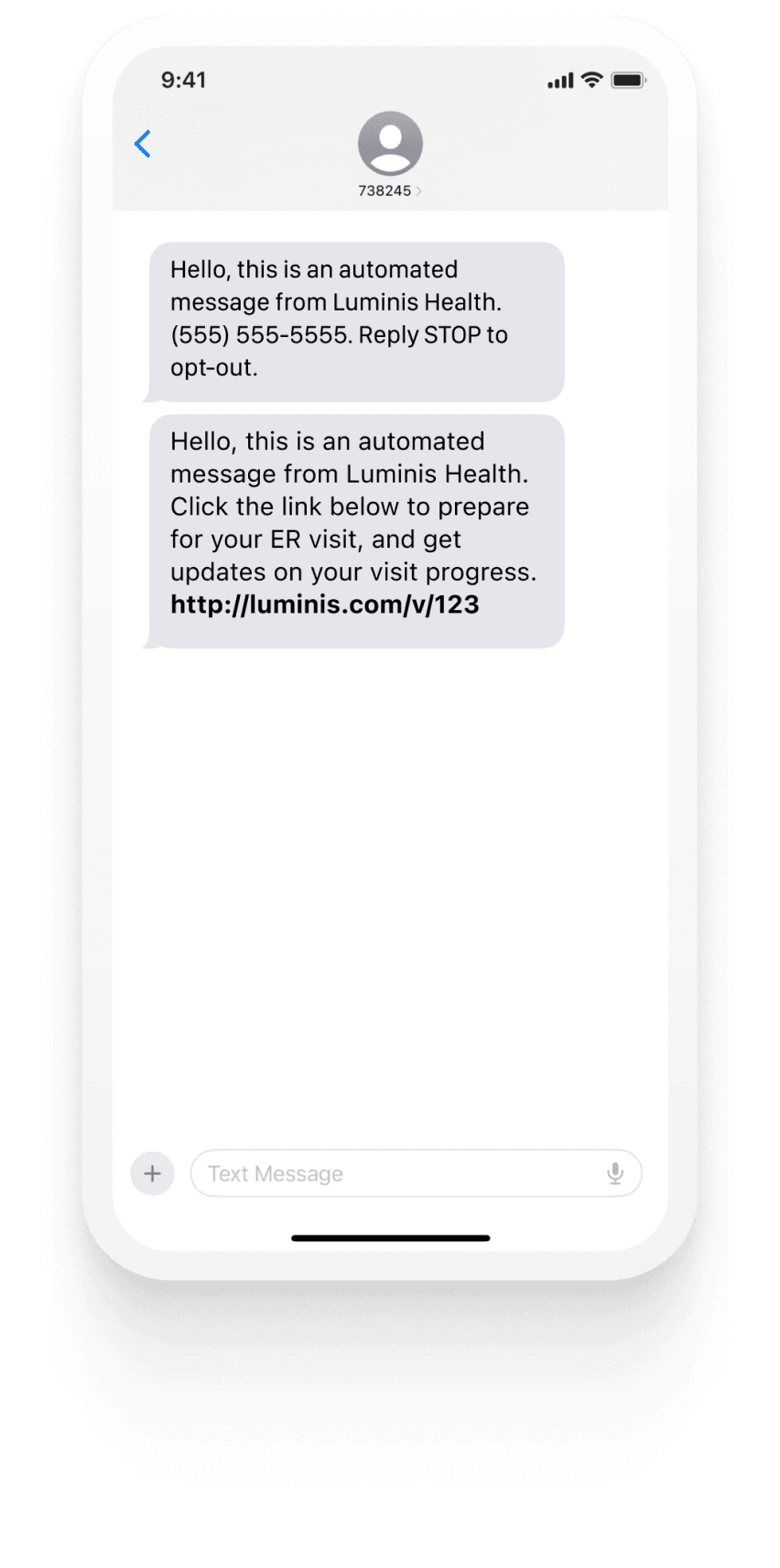
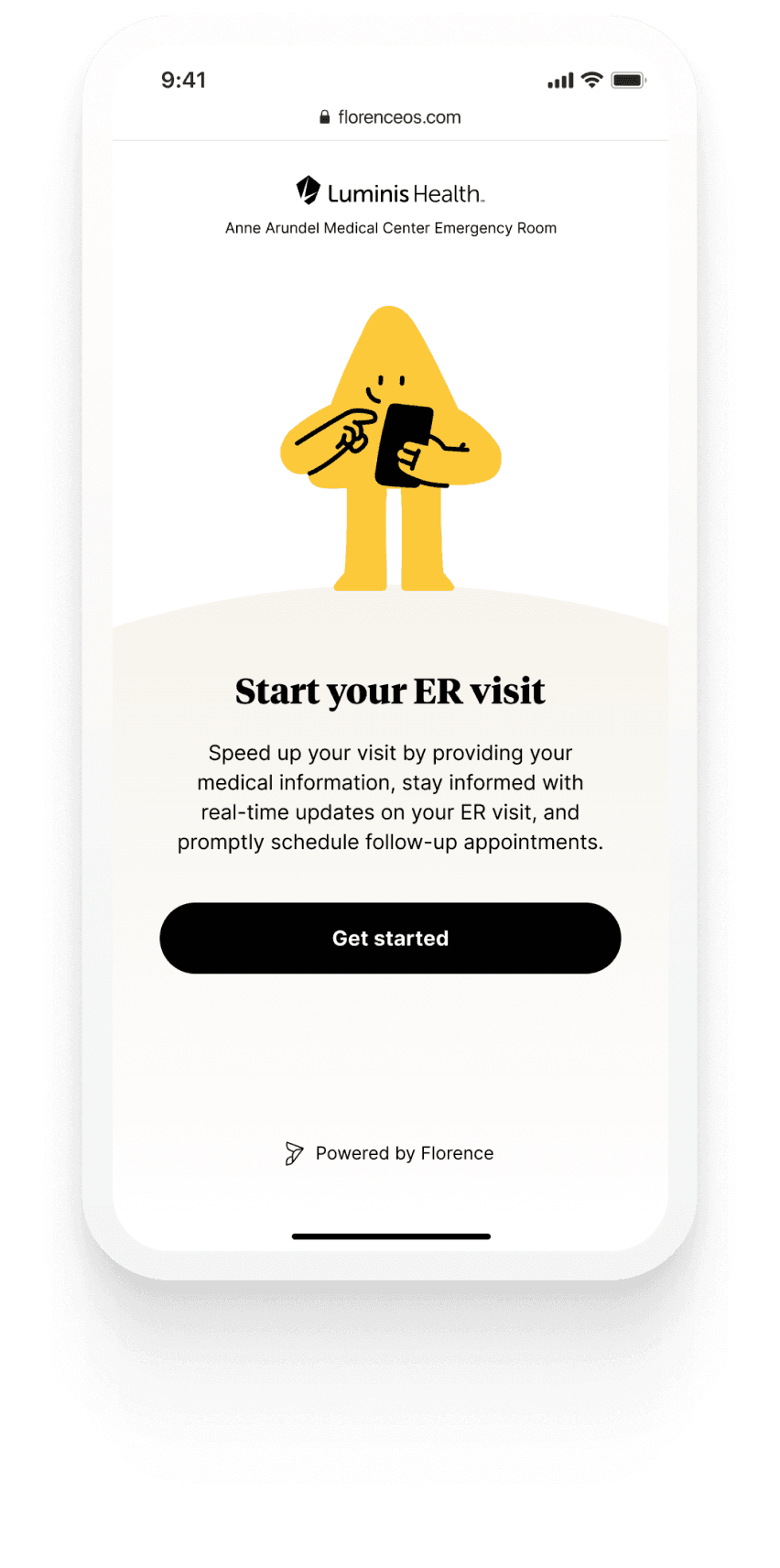
Pre-arrival check-in by SMS.
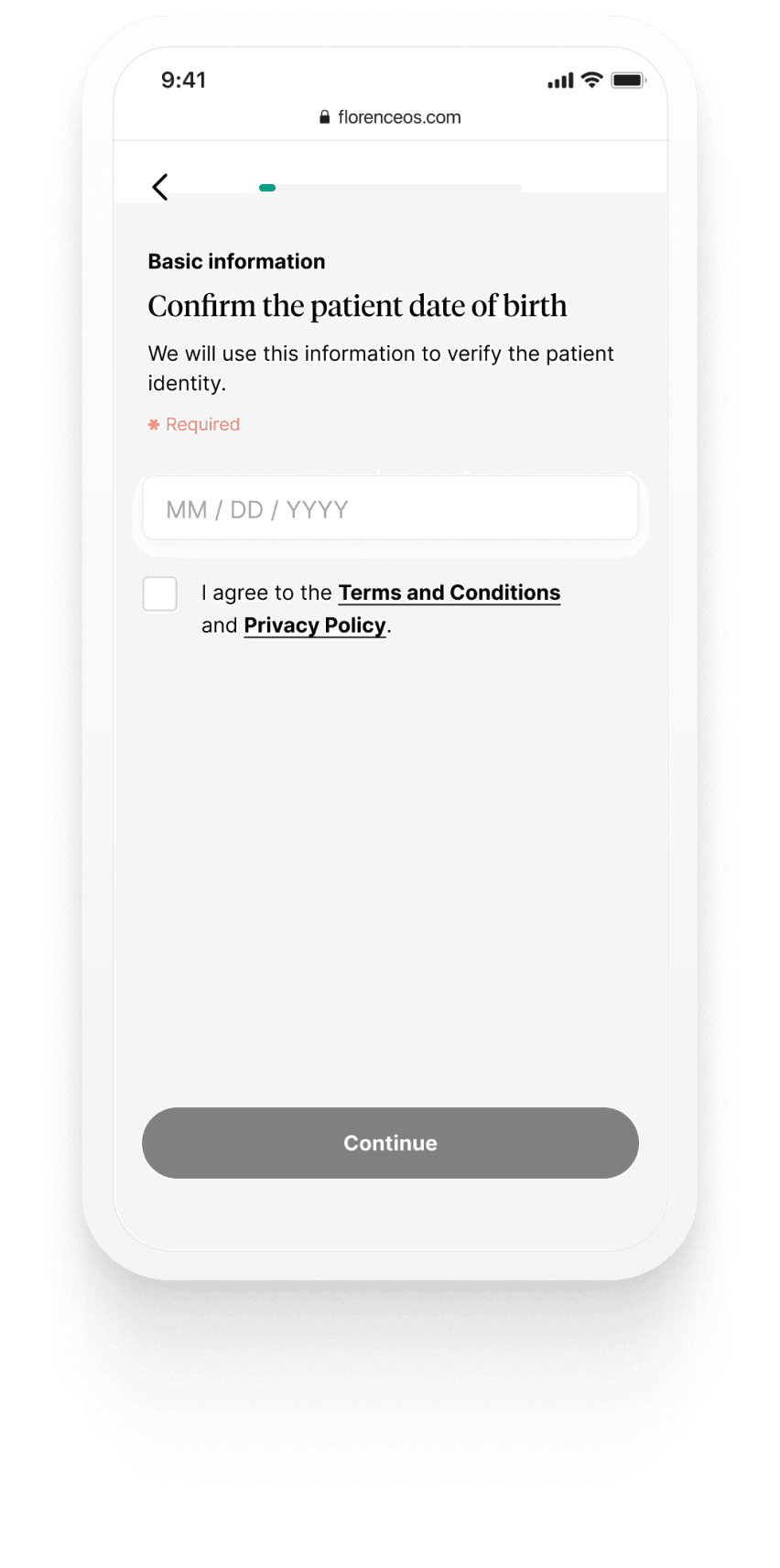
ERG reached patients before they set foot in the ER. A single SMS from Luminis Health dropped a link into their phone, opened a branded welcome, and walked them through ID verification in one tap.
02 · Answers → Re-asking the same 12 questions erodes trust
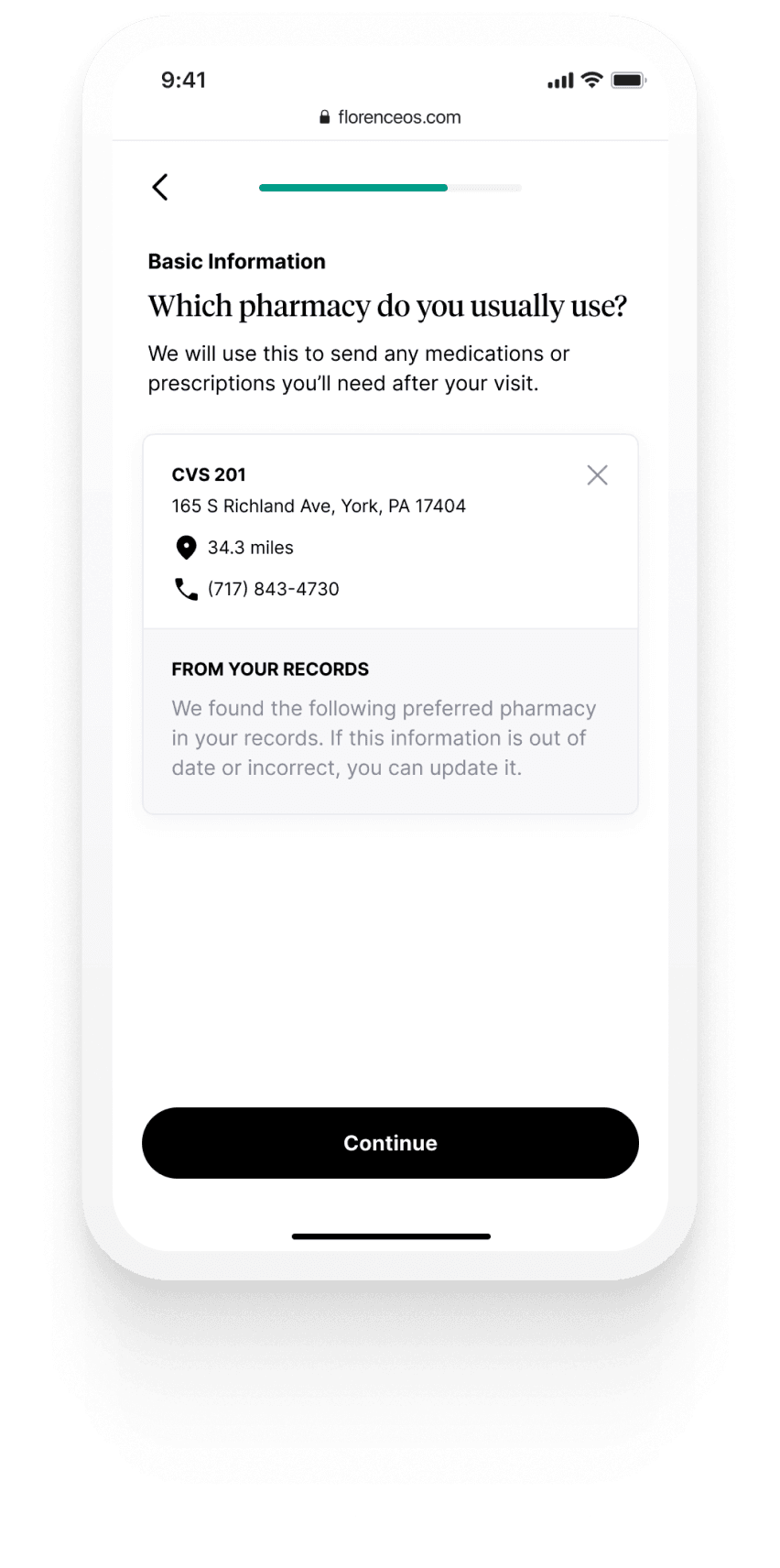
Confirm, don't re-ask.
Rather than ask patients what the hospital already knew, we prefilled the intake from the EHR and asked them to confirm. That single shift, from "type it in again" to "is this still right?" changed the tone of the entire intake.
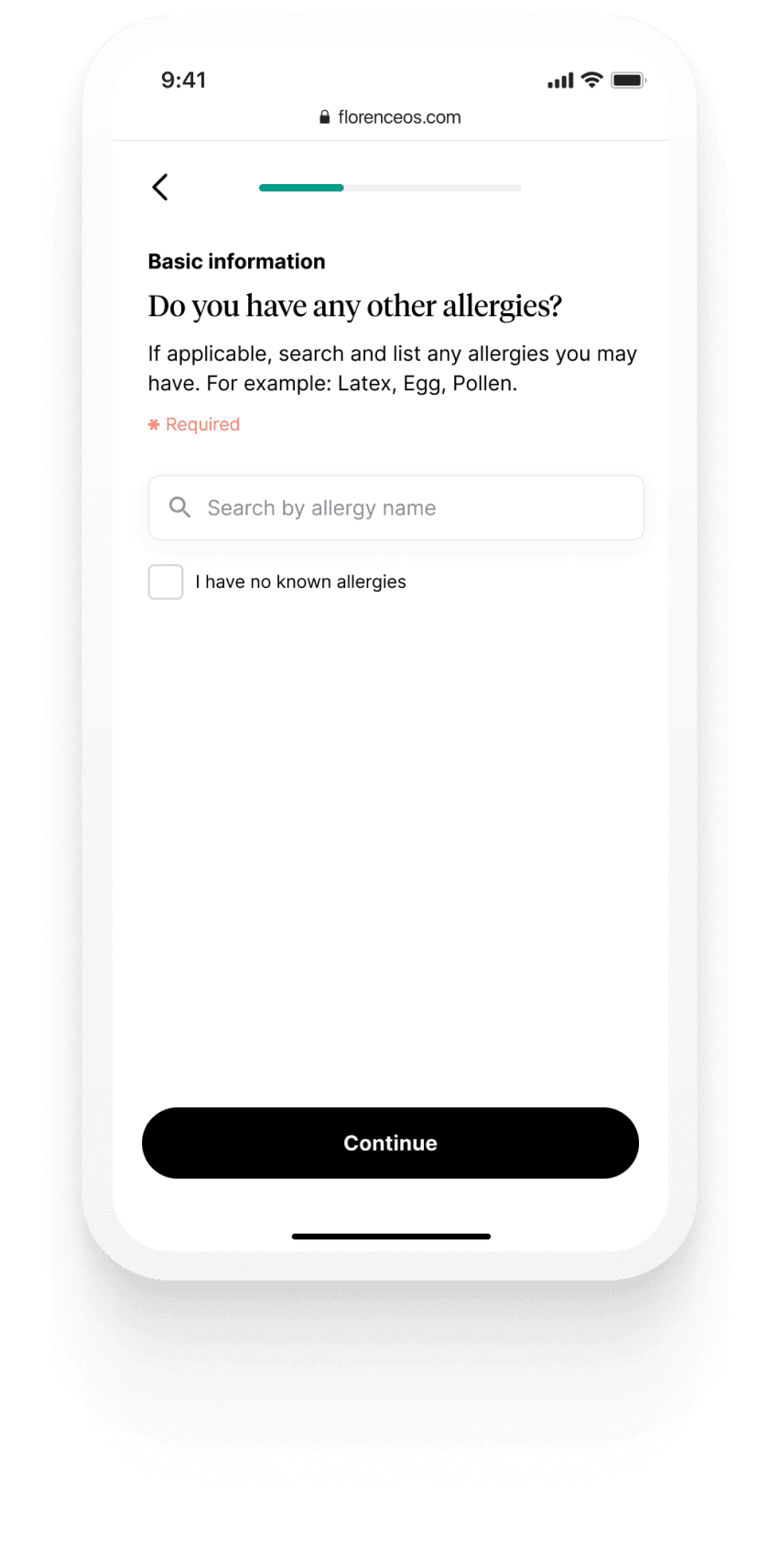
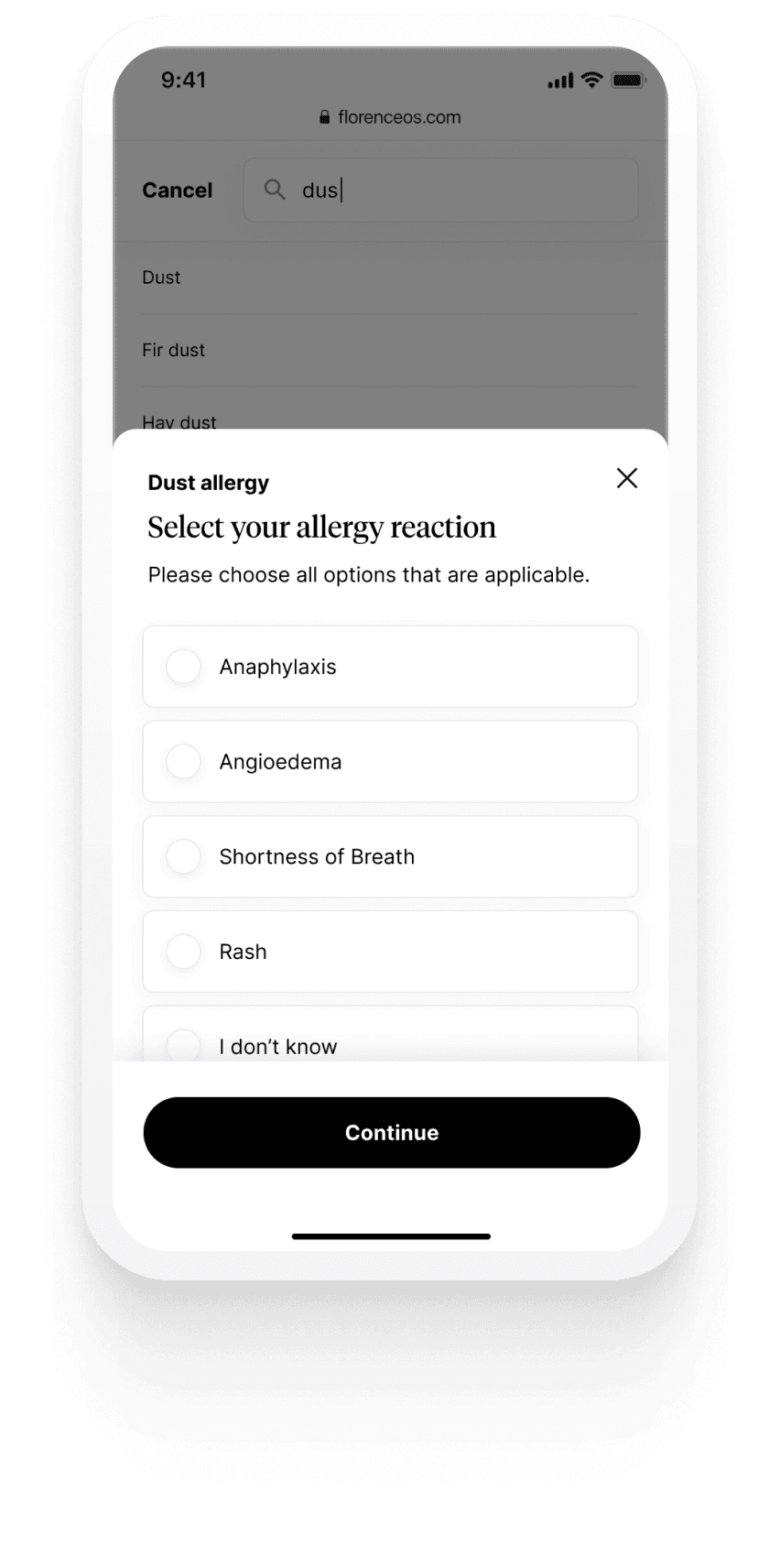
03 · Answers → Nurses didn't have time to ask
Move context capture to the patient side.
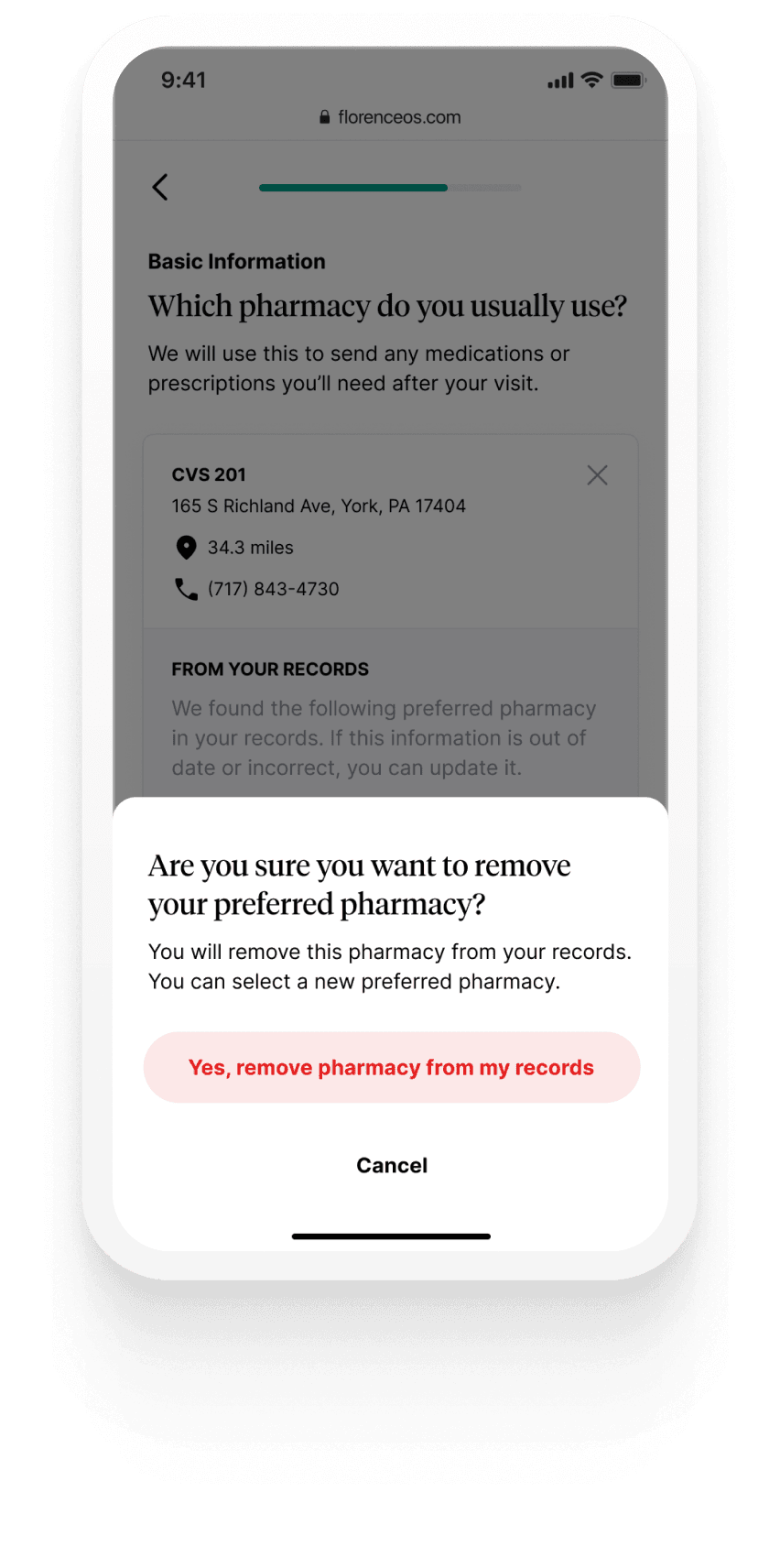
Allergies, reactions, symptom history… the data nurses most often told me they wished they had, and most often didn't. We moved that capture to the patient side, during the wait, backed by clinical databases. Nurses received structured data instead of dictation.
04 · Answers → The quietest question in the waiting room
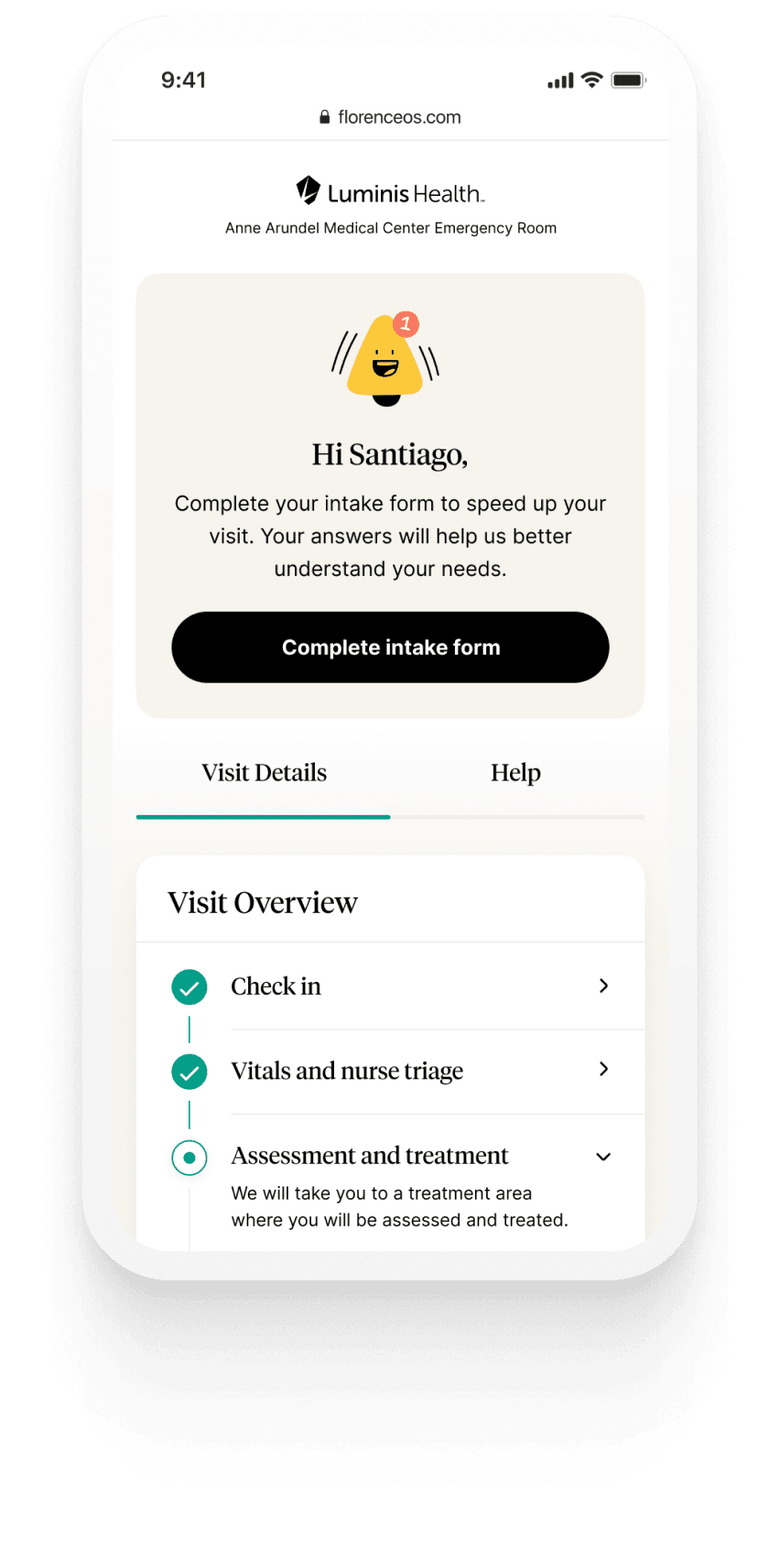
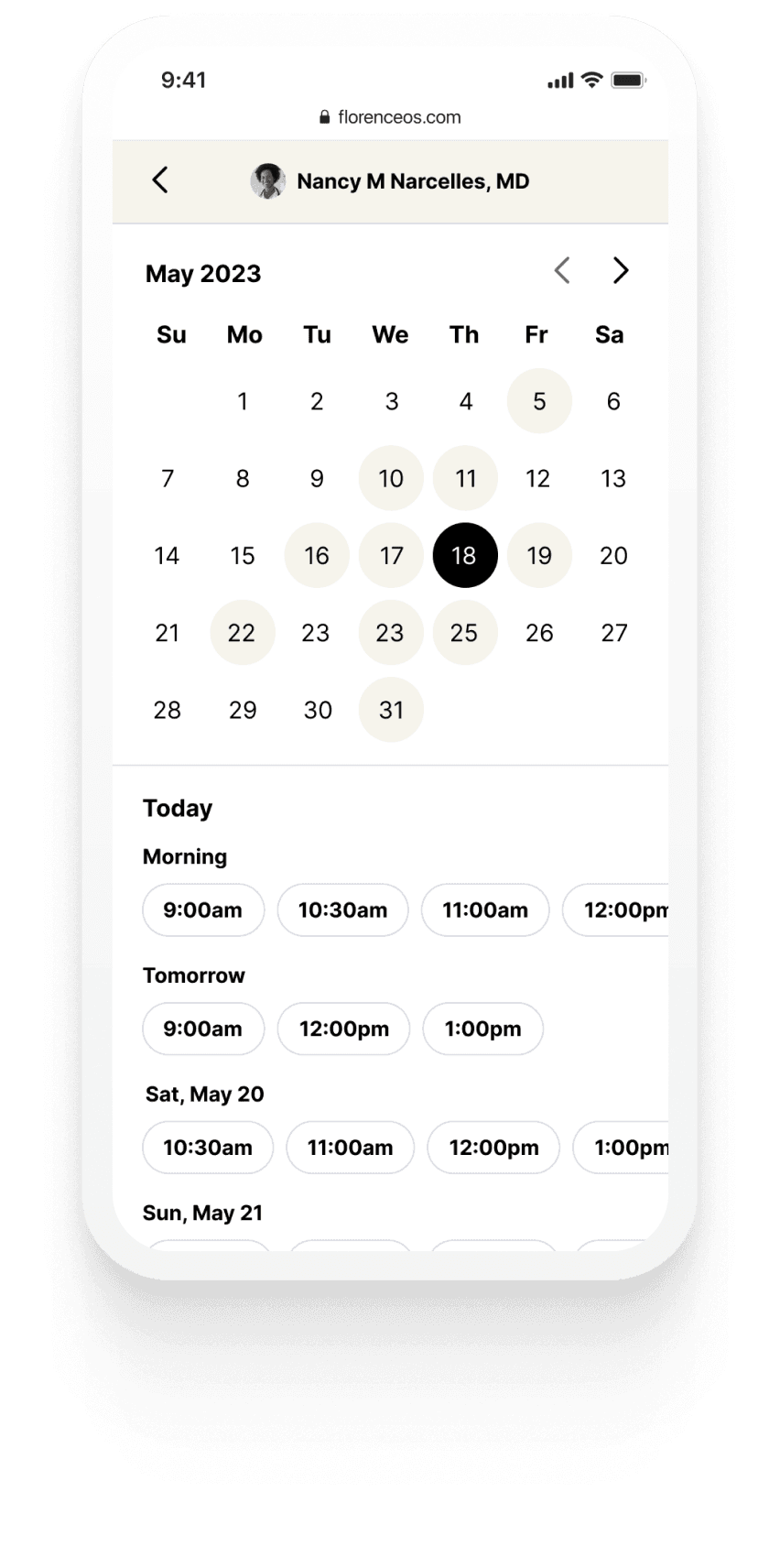
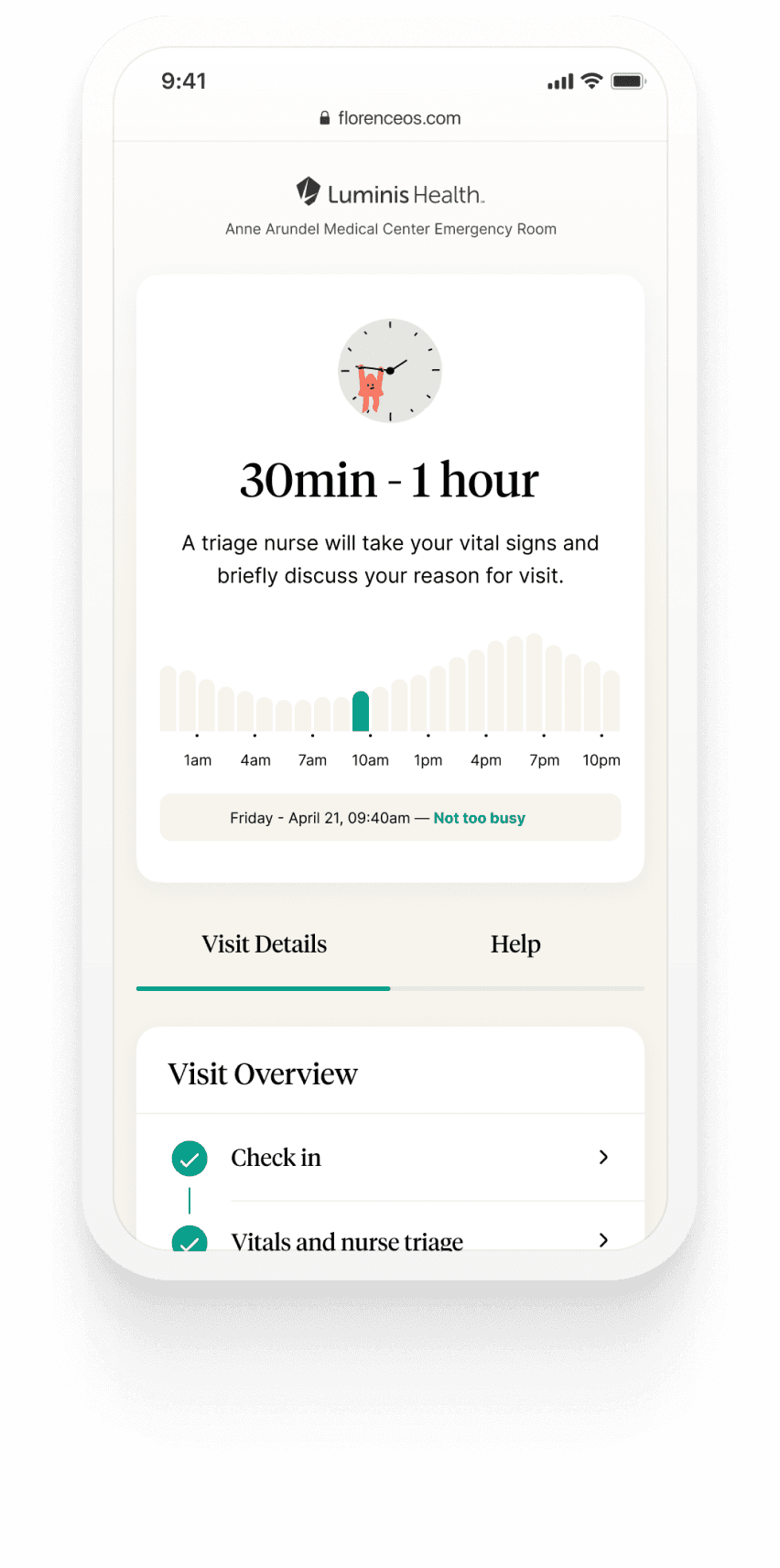
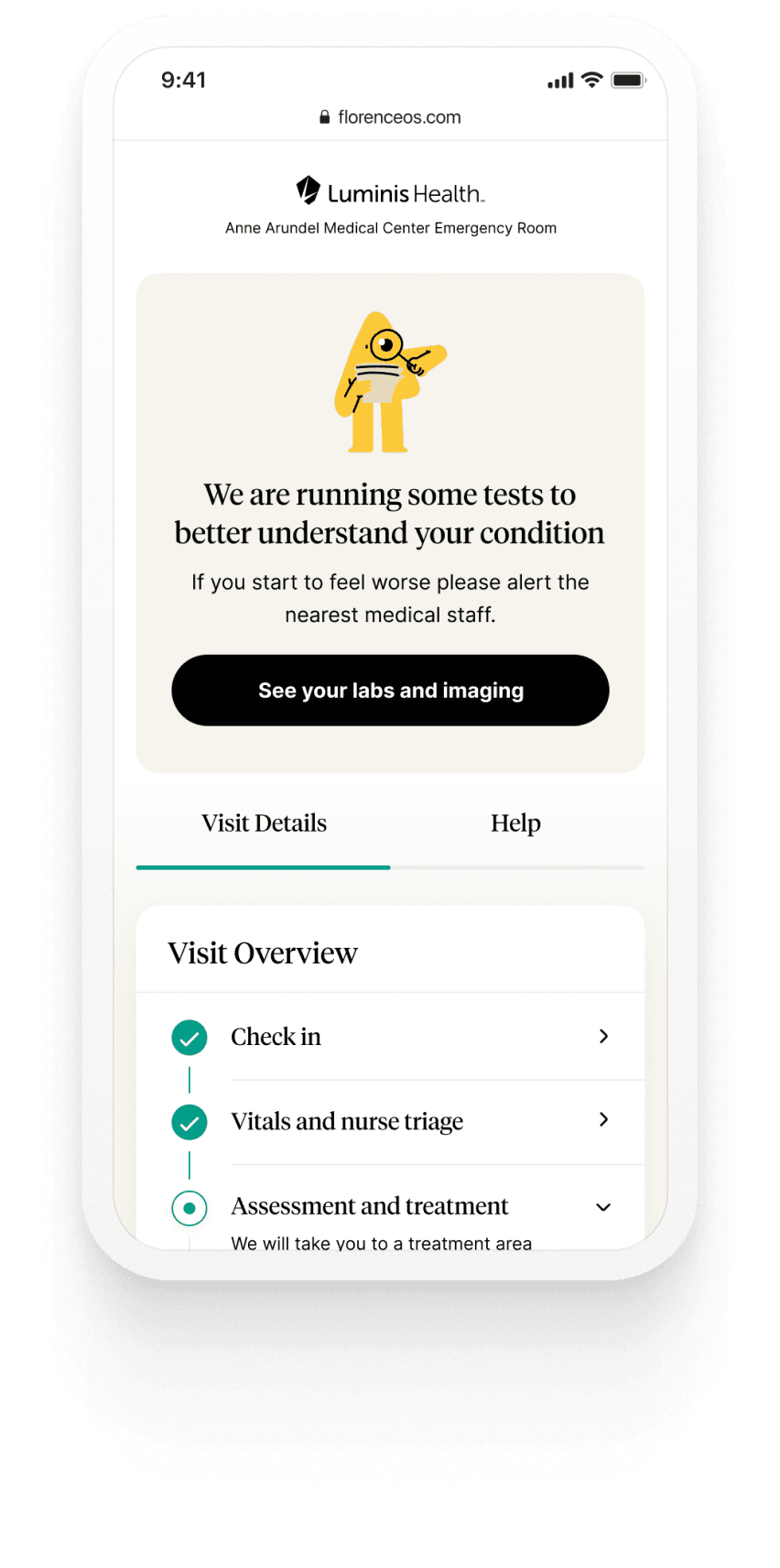
A real timeline, with named steps.
This was the single most important screen in the app, it answered the question nobody was asking out loud: am I still on the list? The timeline showed real, named steps in a patient's visit as they happened. No estimates we couldn't honor.
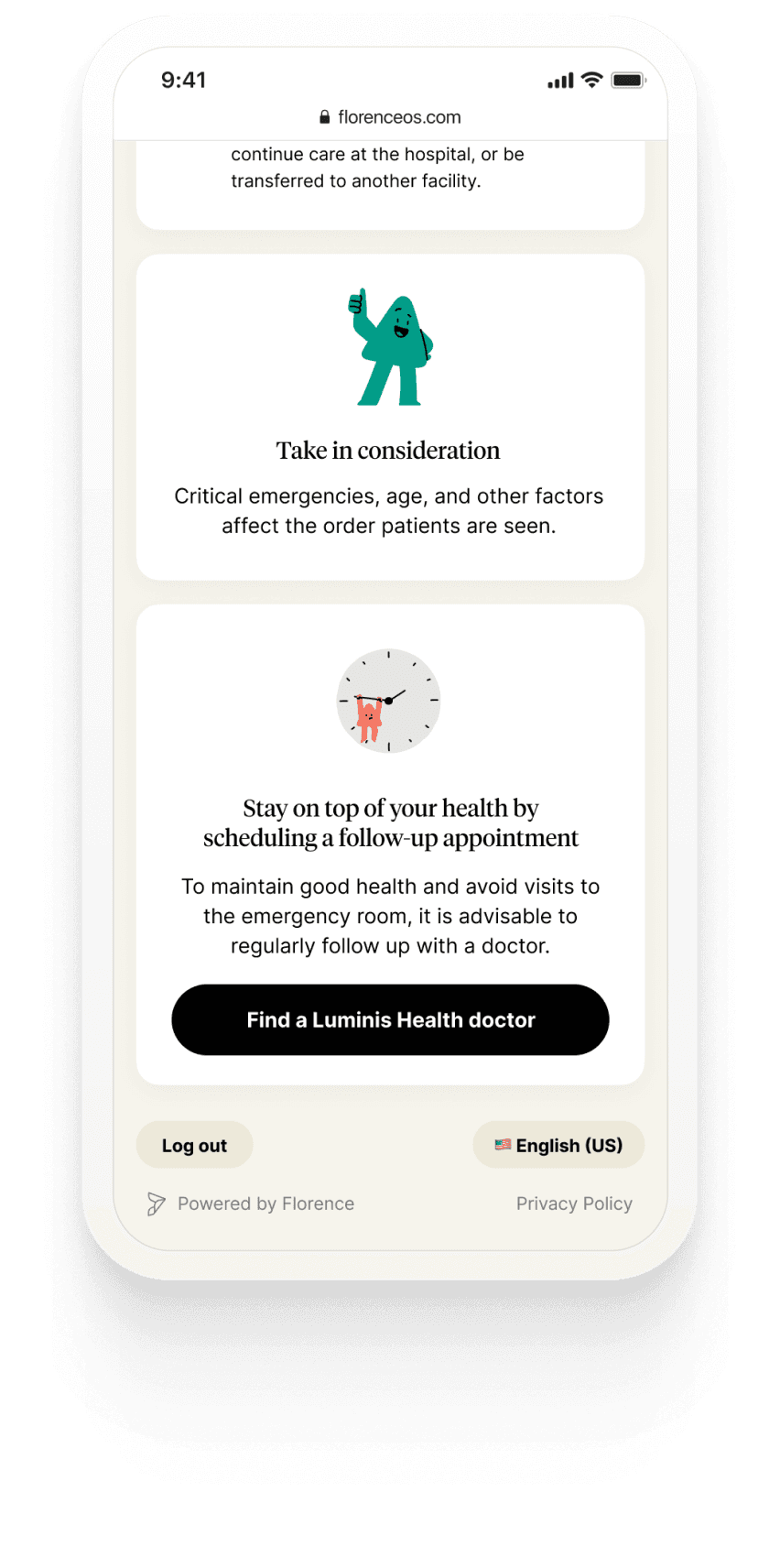
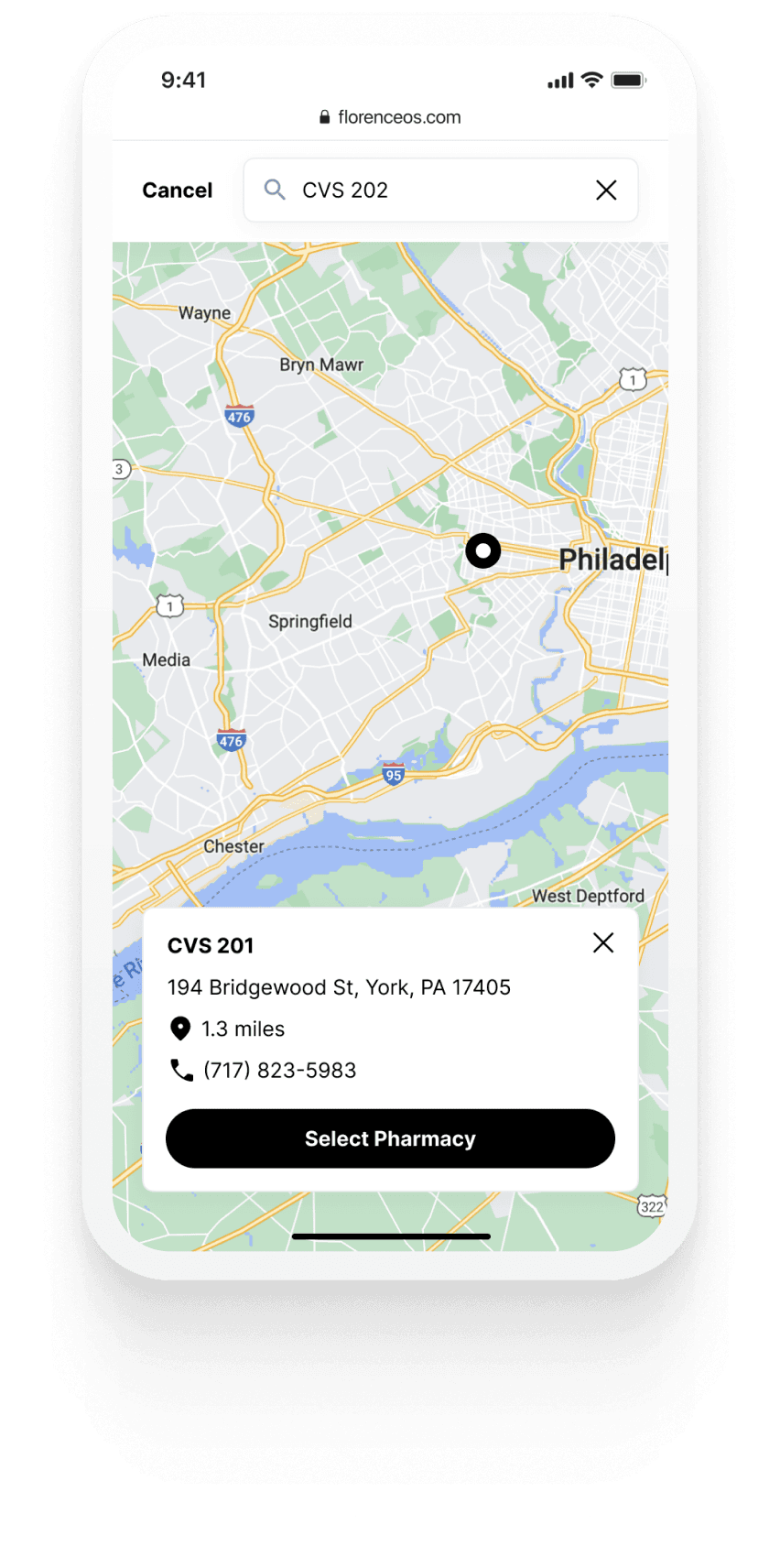
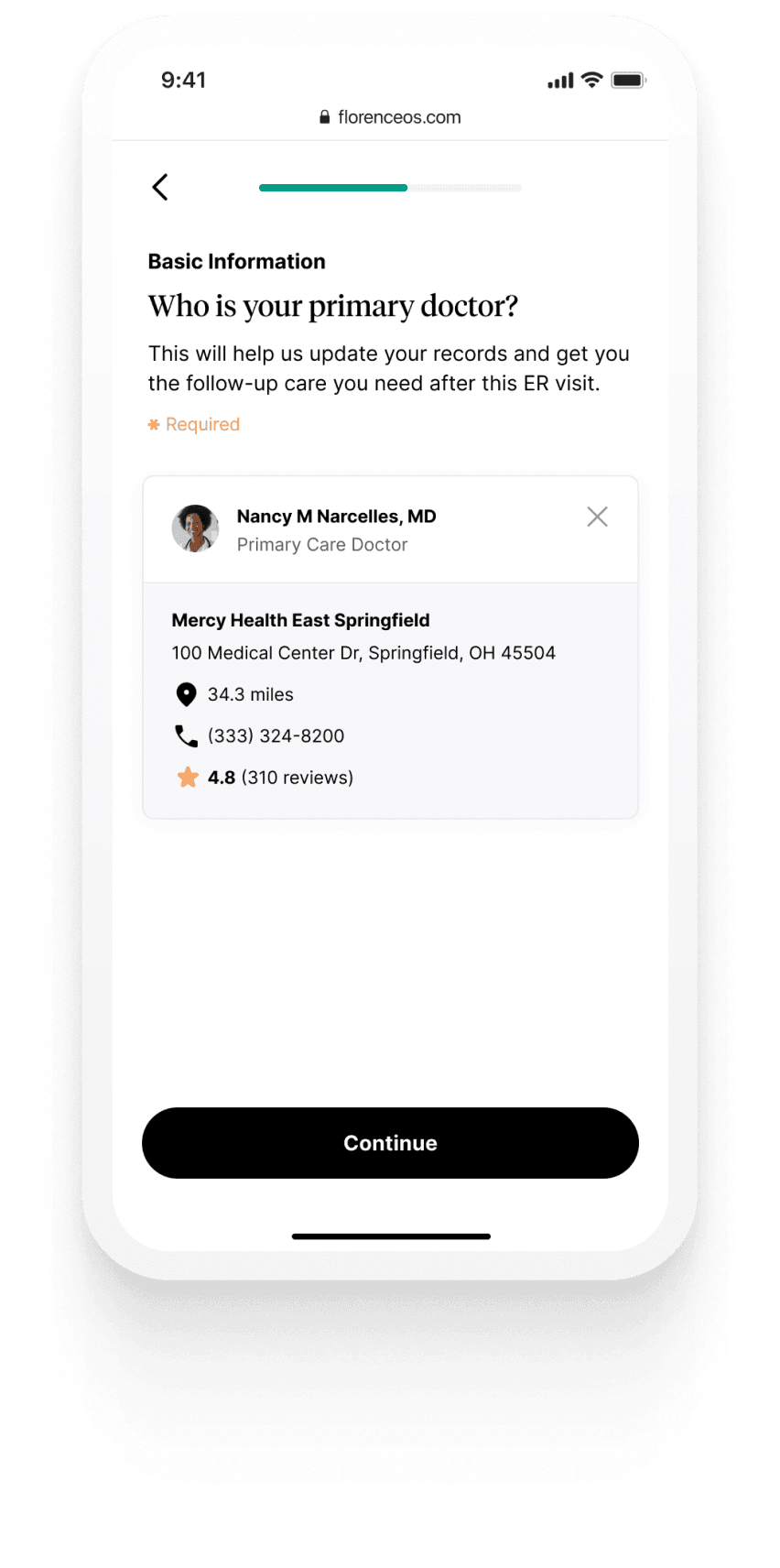
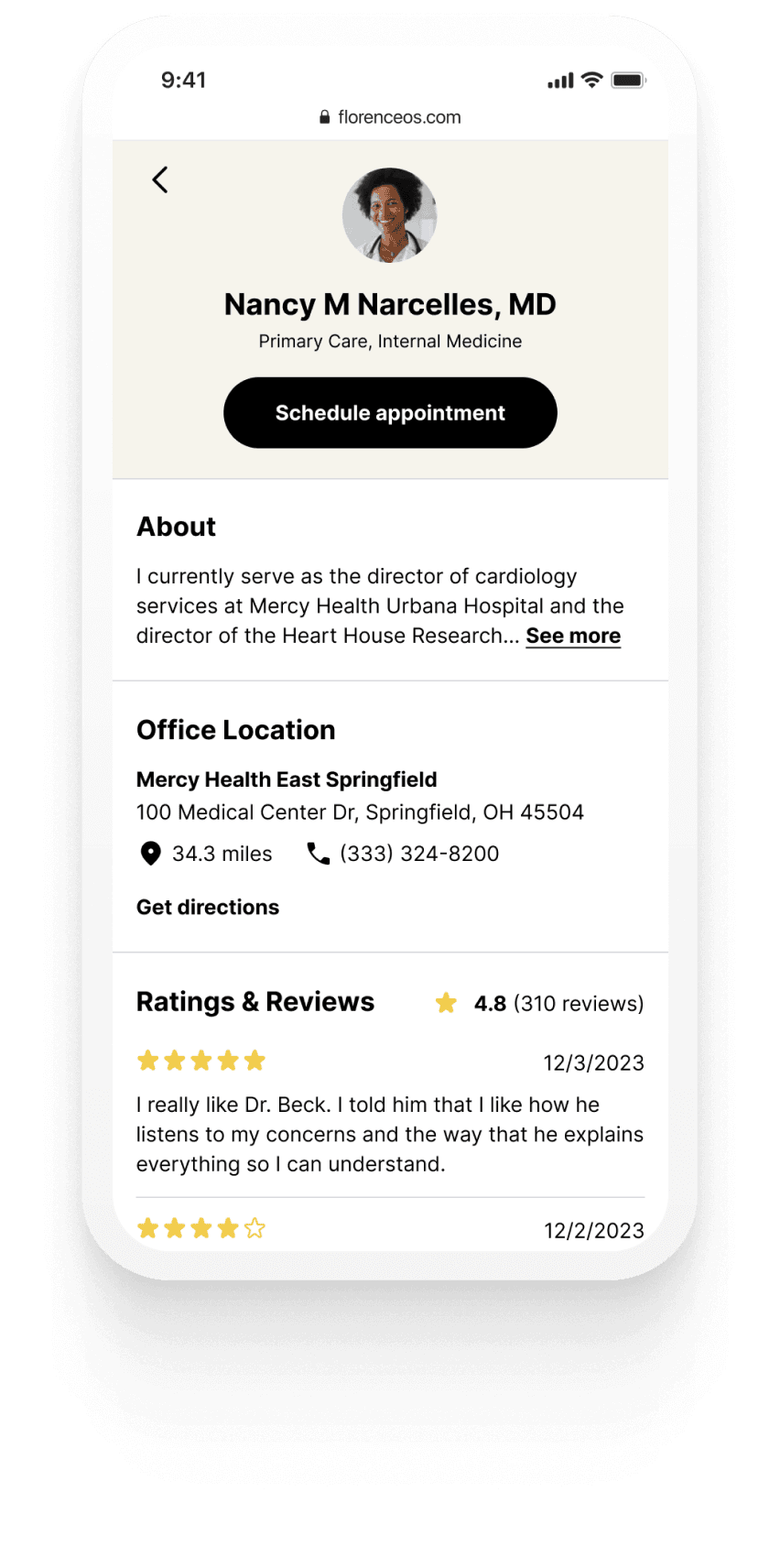
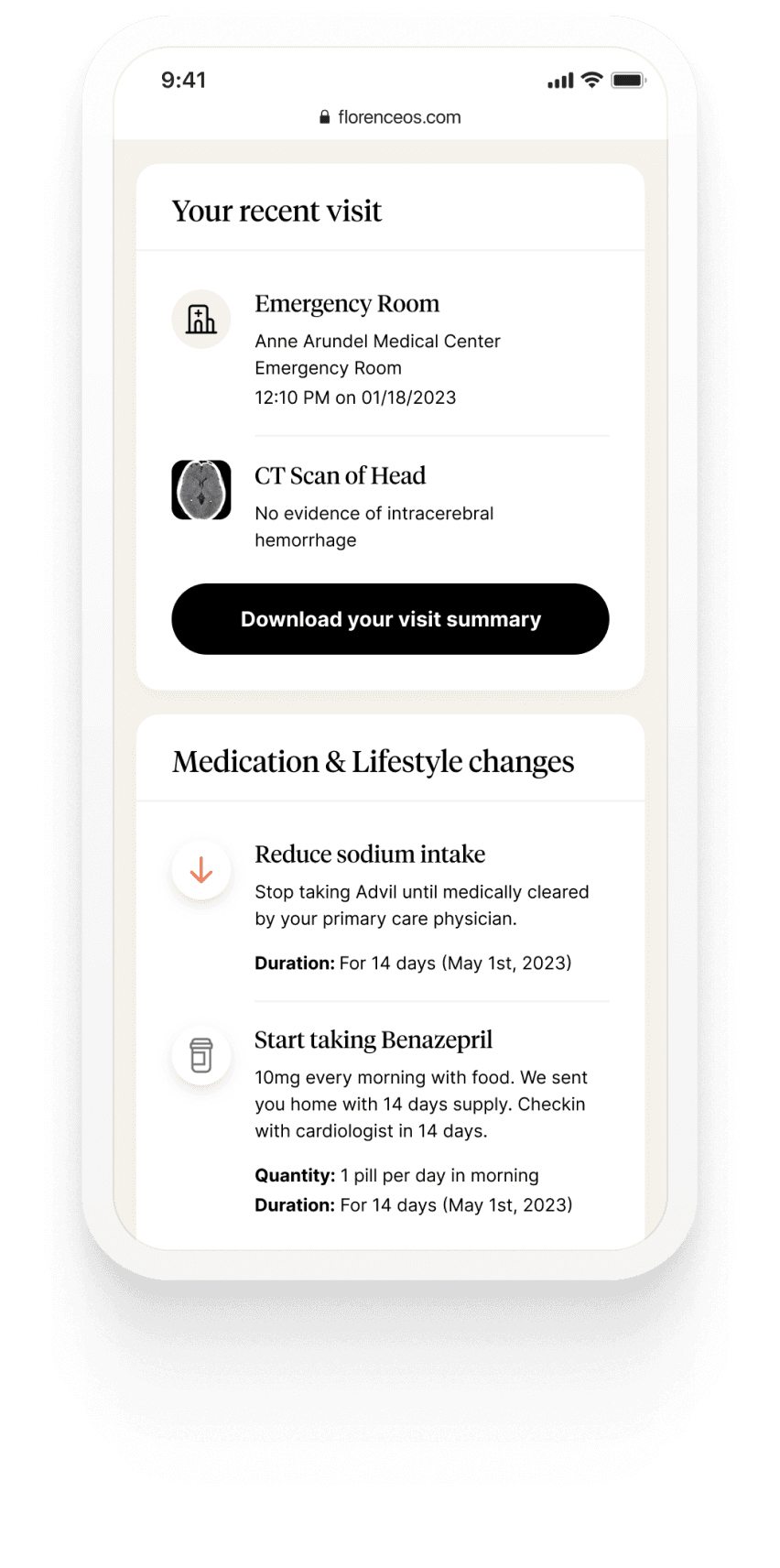
05 · Answers → Discharge with no next step
Attach a PCP in two taps.
At discharge, patients could search for and attach a Primary Care Provider in two taps, with the idea of reducing the chance they'd come back to the ER for something a PCP could handle. A small flow with a big downstream effect.
The Graveyard
What we killed, and why killing it was the design decision.
Every feature on this list made the whiteboard. None of them made it into the app. The ER punished three assumptions we initially thought were safe, and walking away from each one was harder than designing the features that shipped.
Killed
Real-time Lab Integrations
Live lab results on the patient's phone was the dream. The reality was an integration maze across integrations, consent flows, and clinical liability. We couldn't make it safe and useful in time.
Delayed
Predictive Wait Times
We wanted to show patients a wait estimate but one incoming stroke could bump you three times. Any number we showed would be wrong often enough to destroy trust.
Killed
Optimized Treatment Plans
Showing patients a "recommended next step" sounds helpful until you ask who's making the recommendation, on what data, with what liability. We shouldn't have been building this.
Design System
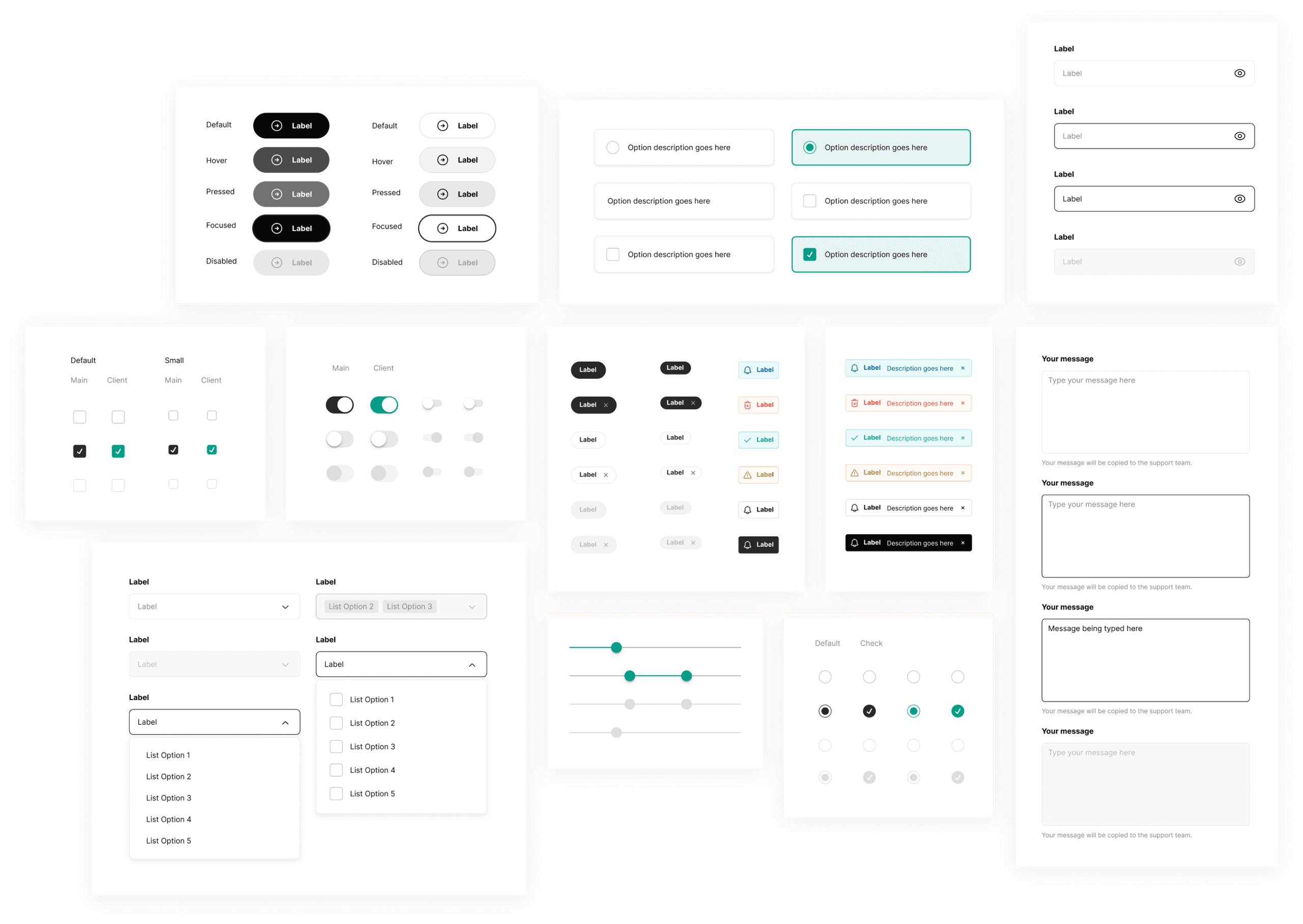
Built for more than one hospital.
ERG's design system was white-label from day one to support multiple health systems. Same design patterns and components rolled into the pediatric ER deployment with minimal rework.
Impact
The number that matters and the one that doesn't.
Across six months of deployment, ERG reached 5,700 patients at three hospitals, including a pediatric ER. The headline stat was a 19-minute reduction in length of stay, roughly 1,800 hours of ER time returned to the system.
Patients who used ERG (Apr–Sep 2023)
Reduction in length of stay
Of ER time returned to the system
Faster nurse intake
The honest reframe
What I'm actually proud of isn't in the dashboard.
The 19-minute number is the headline. The thing that actually moved me was watching a mom in the pediatric ER stop pacing because the timeline showed her her son was about to be seen. That's not a metric — but I think it's the part of the work that mattered.
Startup metrics don't fit here.
Everything I'd learned about measuring product success — activation, retention, NPS, time-to-value — bends or breaks in an ER. You can't NPS a stroke. You can't A/B test triage. The classic playbook is the wrong playbook.
The ER is a battlefield.
No workflow survives it intact. You design for flexibility, not control, and you accept that some parts of the experience are just going to suck because that's the nature of the room.
Sometimes the win is psychological.
Patients felt like progress was being made — even when clinically, nothing had changed. That's not a metric. But it might be the thing that actually mattered.
The honest ending
We had an impact. Just not the one we walked in hoping for.
The original thesis was to buy a hospital and rebuild healthcare from first principles. We didn't do that. The ER was supposed to be the proof — and it was, but it was also a humbling lesson in how much of healthcare is structural, not designable.
Testimonial
“As one of the busiest emergency departments in the country, our nurses and administrative staff immediately saw the benefit of Florence. Nurses are saving time and seeing patients faster in our ED. Patients appreciate the modern, transparent experience and the ability to share their visit with family.”
Saad Chaudhry
Chief Digital & Information Officer, Luminis Health